Capsule Endoscopy
Obscure Gastrointestinal blood loss and iron deficiency anaemia
Capsule Endoscopy | Pill Cam | wireless video capsule
Capsule endoscopy, or “Pill-Cam” is a procedure used to diagnose and monitor diseases of the small intestine with a small, disposable, pill sized camera. Dr Prematilake uses the Given imaging PillCam SB3, the next generation HD capsule that provides exceptional image quality and diagnostic confidence that comes with a pill that has been used more than 3 million times worldwide. PillCam SB3 is the only capsule licensed for use in both adults and children as young as 2 years old.
Where is the small intestine (small bowel)?
The small intestine starts after the stomach and comprises the 4 parts of the duodenum, the jejunum and the ileum. It measures close to 3 times of your height. Gastroscopy examines the oesophagus, stomach and first two parts of the duodenum, while colonoscopy examines the entire large bowel (colon) and up to 10cm of the terminal ileum. Capsule endoscopy examines the rest without the need for hospitalization or sedation.
How is it done?
Capsule endoscopy uses a vitamin sized capsule which contains a tiny HD camera, batteries, LED light and transmitter. The capsule is swallowed with a sip of water and travels through the entire intestine taking 2 to 6 images per second. By the end of the procedure up to 100,000 images may have been captured and transmitted to a data recorder that is worn around the waist the entire time.
Why is it done?
Capsule endoscopy is used to locate possible sources of bleeding within the small intestine when gastroscopy and colonoscopy have excluded blood loss from another location. Common indications include iron deficiency anaemia, unexplained melaena (black tarry motions due to altered blood) and obscure abdominal pain. The procedure can be used to exclude and to track small bowel tumours and to determine the severity of Crohn’s disease of the small intestine. I have picked up 3 small bowel tumours which would have been missed till late if this was not available.
Preparing for the procedure
The preparation for the procedure is very easy and details are available from the Clinic.
What happens during the procedure?
On the day of the procedure you will need to come to my rooms in Taree at 8 am. . A glass of water is permitted when swallowing the capsule and a substance called ‘simethicone’ is added to this to prevent ‘bubbles’ which can interfere with the picture transmitted by the capsule. Just prior to swallowing the capsule you will also take a tablet of metaclopromide (maxolon/pramin) which helps the capsule to leave the stomach. Please let us know if you are allergic to this medication and it will be avoided. On the day of the procedure, a harness, holding the data recorder, is worn for 8 hours after the capsule is swallowed. Gentle activity is encouraged while wearing the harness as this will aid the progress of the capsule. No fluids should be taken for 2 hours after the capsule is swallowed and solid food is not permitted to be eaten for 4 hours afterwards. Do not swallow chewing gum during the examination. You will be instructed to come to Taree or Forster depending on your home town.
What happens after the procedure?
Eight hours after the capsule is swallowed, you will return to the Clinic to have the belt removed. The information from the data recorder is downloaded onto a computer and the images are composed into a video to be examined by the doctor. The capsule is single use only and does not need to be retrieved. The capsule passes naturally in a stool within 1-3 days. Most patients are not aware it has passed. The capsule doesn’t need to be retrieved and can be safely flushed down the toilet.
Are there any risks?
Capsule endoscopy is a very safe procedure. Complications of capsule endoscopy are very infrequent. The capsule has a gel coating which makes it easy to swallow. Less than 1 patient in 100 has difficulty swallowing the capsule. Approximately 1 in 100 patients retain the capsule in the bowel. This may occur if the bowel is narrowed or has some other unusual anatomy. Usually the capsule will eventually pass. On rare occasions it will need to be removed endoscopically or surgically. The obstructing lesion can be corrected at the same time. If bowel narrowing is suspected your doctor may suggest an initial trial with a dissolvable (Patency) capsule. On the day of the test, approximately 1 in 10 patients may have a slow small bowel transit and the capsule may not be seen to reach the large bowel. An abdominal X-ray may then be arranged to check that the capsule has passed out of the bowel. While wearing the harness and data recorder we advise you to stay away from large radio transmitters (e.g. TV transmission towers) and not to visit airports where the harness could trigger security screening equipment. You must not have an MRI scan until the capsule has passed from your body.
Capsule endoscopy is currently reimbursed by the MBS (Medicare) for the investigation of obscure gastrointestinal blood loss following prior gastroscopy and colonoscopy, and monitoring of Peutz-Jager Syndrome.
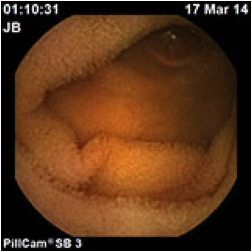
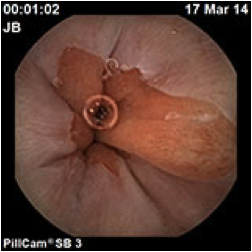
Normal GI anatomy as seen through the Capsule